Cardiovascular medications
Beta-blockers, calcium channel blockers
- Pre-surgery
- Can take usual dose on the morning of the surgery with sips of water with at least a 2 hour window before surgery
- B-blocker should not be initiated within 24 hours before non-cardiac surgery
- But if a patient is already taking it chronically, then the patient should continue taking it during the perioperative period
- If patient’s SBP is low prior to surgery then it is also acceptable to reduce or lower the dose of beta-blocker for the day of the surgery
- Post-surgery
- After surgery, patient can be given beta-blocker via IV until patient is able to take it orally
ACEi/ARBs
- What are we worried about?
- Intra- and post-operative hypotension
- Highest risk for post-operative hypotension is 24 hours after surgery
- Pre-surgery
- Hold ACEi/ARBs 24 hours before non-cardiac surgery
- Post-surgery
- After surgery, patient can be given ACEi/ARB on post-operative day 2 so long as patient is
- Hemodynamically stable
- Taking medications PO
- After surgery, patient can be given ACEi/ARB on post-operative day 2 so long as patient is
Diuretics, K supplements
- What are we worried about?
- Intra- and post-operative hypotension
- Hyperkalemia
- Pre-surgery
- If patient is only taking it for hypertension, or for heart failure with a controlled volume status, diuretics should be held the day before surgery
- If potassium wasting diuretics are being held, attention should be paid to K levels, with the possible consideration to also discontinue KCl
- Post-surgery
- After surgery, patient can be given diuretics and KCl as soon as they are able to take medications PO
Statins, niacin, fibrates
- Pre-surgery
- Non-statin meds should be stopped the day before surgery
- Statin should be continued perioperatively
- Post-surgery
- Any cholesterol medications stopped the day before surgery can be resumed as soon as the patient is back on a regular diet
Nitrates
- What are we worried about?
- Intra- and post-operative hypotension
- Pre-surgery
- Sublingual nitroglycerin acceptable right up to the administration of anesthesia
- During surgery nitroglycerin should be administered via nitropaste (topical application)
- Post-surgery
- After surgery, can resume PO nitroglycerin as soon as he can take medications orally
Amiodarone
- Pre-surgery
- Hold the night before surgery
- Post-surgery
- After surgery, can resume amiodarone as soon as the patient can take medications orally
Digoxin
- Pre-surgery
- Can take usual dose on the day of the surgery with sips of water with at least a 2 hour window before surgery
- Post-surgery
- After surgery, patient can be given digoxin via IV until patient is able to take it orally
Antiplatelet and anticoagulant medications
Anticoagulants
- What are we worried about?
- Bleeding risk (especially in cardiac surgery and neurosurgery)
- Pre-surgery
- DOACs can be stopped 2-3 days prior to a procedure
- Warfarin can be stopped 5 days prior to a procedure
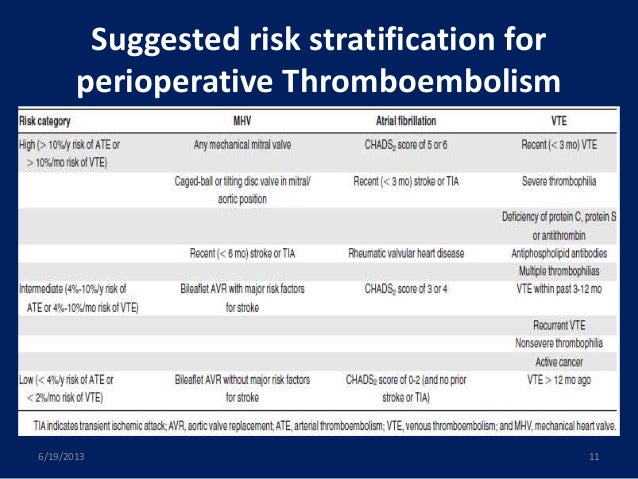
- Depending on the thrombotic risk profile of the patient, for patients who chronically take warfarin, bridging anti-coagulation may be provided in order to minimize the time the patient is not being anti-coagulated
- Bridging is typically conducted using LMWH or unfractionated heparin and is performed both pre-operatively and post-operatively (as patients are taken off of warfarin before surgery and then put back on warfarin after surgery)
- Bridging with LMWH or UFH is done 2 days after stopped heparin but 3 days before the surgery (which is why it is important that wafarin is stopped 3 + 2 = 5 days before the surgery)
- Look up risk stratification guidelines when deciding whether to bridge warfarin
- See BRIDGE trial
- LMWH is generally held 24 hours before the procedure
- If LMWH is twice daily injection then the evening dose is held
- If LMWH is once daily injection then only 1/2 of the total daily dose is provided as a morning injection the day before the surgery
- UFH
- Remember UFH has a short half life (45 minutes) and is often given as a continuous infusion in contrast to LMWH which is often given as subcutaneous injection
- The IV infusion of UFH is held 5 hours before the surgery
- Post-surgery
- After surgery can resume warfarin without LMWH or UFH as long as INR is within the therapeutic range; however LMWH or UFH cannot be started immediately post-OP
- Bridging LMWH or UFH can be started 24 hours after a minor procedure
- Bridging LMWH or UFH can be started 48-72 hours after a major procedure
- After surgery can resume warfarin without LMWH or UFH as long as INR is within the therapeutic range; however LMWH or UFH cannot be started immediately post-OP
{kind=link}
ASA/clopidogrel
- What are we worried about?
- Bleeding risk (especially in cardiac surgery and neurosurgery)
- Pre-surgery
- Should be stopped 7-10 days before surgery (at the very least 3 days before surgery) EXCEPT in patients with a recent coronary artery stent and patients undergoing carotid endarterectomy
- Post-surgery
- After surgery, can resume ASA as soon as major bleeding risk has subsided (around 8 days for major non-cardiac surgery)
Pulmonary medications
Inhaled bronchodilators
- Pre-surgery
- Can be continued perioperatively including on the day of surgery
Leukotriene inhibitors
- Pre-surgery
- Can be continued perioperatively including on the day of surgery
- Post-surgery
- After surgery, can be resumed once patient is able to take medications orally
Inhaled and systemic corticosteroids with pulmonary disease
- What are we worried about?
- Deterioration in lung function
- Adrenal insufficiency due to abrupt withdrawal
- Pre-surgery
- Can be continued perioperatively
Gastrointestinal medications
H2 blockers and PPIs
- What are we worried about?
- Aspiration of gastric contents
- Stress ulcers
- Pre-surgery
- Patients chronically on H2 blockers and PPIs can remain on them during the perioperative period
Endocrine medications
Thyroxine
- Pre-surgery
- Can take usual dose on the morning of the surgery with sips of water with at least a 2 hour window before surgery
Oral contraceptives and Hormone Replacement Therapy
- What are we worried about?
- DVT risk with estrogen containing contraceptives
- Pre-surgery
- Hold oral contraceptive 4 weeks before major surgeries
- Post-surgery
- After surgery, can resume medication when fully ambulatory
Glucocorticoids
- What are we worried about?
- Risk of infection and ulcer associated with glucocorticoid-associated immunosuppression
- Pre-surgery
- Lowest possible dose of glucocorticoids should be used in the perioperative period due to risk of infection
- If dose of glucocorticoid is higher than the equivalent of 10 mg of prednisone, then the patient’s disease is not actively controlled and if possible surgery should be delayed until prednisone dose can be lowered safely
- Post-surgery
- After surgery, can resume PO steroids as soon as patient can take medications orally
Oral hypoglycemics
What are we worried about?
- What are worried about?
- Risk of hypoglycemia and lactic acidosis with metformin
- Pre-surgery
- Metformin – hold 48 hours before surgery
- Acarbose – hold night before surgery due to GI side effects
- DPP4 inhibitors – avoid on day of surgery due to increased risk of aspiration related to delayed gastric emptying
- Sulfonylureas/meglitinides/thiazolidinediones – can continue perioperatively
- If on any oral hypoglyemic not listed above, then you can discontinue it the night before surgery and place the patient on IV or SQ insulin
- Post-surgery
- After surgery, patient can be placed on insulin until they can eat food by out and then they can be switched back to their oral hypoglycemic
Pain medications
NSAIDs
- What are we worried about?
- Risk of bleeding and intraoperative renal injury
- Pre-surgery
- Hold 2-3 days before surgery
- Post-surgery
- After surgery, can resume after hemodynamic stability is achieved, renal status returns to baseline and bleeding risk is decreased
Opioids
- What are we worried about?
- Withdrawal associated with abrupt discontinuation
- Pre-surgery
- In chronic users, opioids should be continued throughout the perioperative period
Neurological medications
SSRIs
- Pre-surgery
- Can take usual dose on the morning of the surgery with sips of water with at least a 2 hour window before surgery
- Post-surgery
- After surgery, can resume as soon as the patient can take medications orally
TCA
- Pre-surgery
- Can be cautiously continued throughout perioperative period
Lithium
- Pre-surgery
- One of two options
- Stop 2-3 days before a major surgery
- Continue perioperatively with close monitoring of electrolytes
- One of two options
- Post-surgery
- Resume when creatinine and electrolytes stabilize
Antipsychotics/Antiepileptics
- Pre-surgery
- Can be continued throughout perioperative period
- Should not be abruptly stopped
Anti-Parkinson
- Pre-surgery
- Sinemet can be continued in perioperative period
- Bromocriptine and pergolide should be held the day of surgery
Benzodiazepines
- What are we worried about?
- Withdrawal associated with abrupt discontinuation
- Pre-surgery
- In chronic users, benzodiazepines should be continued throughout the perioperative period
Herbal medications
- Pre-surgery
- Stop 1-2 weeks before surgery
- Post-surgery
- Herbal products may be resumed after patient is discharged from the hospital