Causes of scrotal pain can be divided into 2 categories: emergency and non-emergency.
Emergency causes of scrotal pain
Testicular torsion
Testicular torsion refers to the acute twisting of the spermatic cord in the scrotum due to improper fixation of the testicle to the scrotal wall. It occurs typically in men younger than 30 years. Bimodal age distribution close to birth and in adolescence/teens.
Testicular torsion is the most concerning item on your differential for acute testicular pain! It is an emergency as permanent damage can occur in as little as 6 of the onset of pain. Get them to exploratory surgery within the 6 hour window.
Clinical presentation
Acute unilateral onset pain associated with radiation to the lower abdomen, nausea and vomiting. History may include triggers such as recent trauma or sexual intercourse.
The testicle that is affected will appear higher (high riding) than the other and will appear swollen and tender to palpation. Absent cremaster reflex will also be seen (with patient standing, pinch or stroke medial thigh and watch for elevation of ipsilateral testicle). Negative Prehn sign will be seen (elevation of testicles providing relief suggesting epididymitis)
Diagnosis
Clinical diagnosis; should be made quickly. Do not wait for U/S or blood work. It is not needed to make the diagnosis.
Management
Patient should be sent to emergency room and then surgical management. Detorsion of testicle should be done as soon as possible to avoid ischemia, infertility and loss of testicle.
Non-emergency causes of scrotal pain
Epididymitis (orchitis if it involves the whole testicle)
Epididymitis involves inflammation of the epididymis most commonly due to sexual or urinary tract infections.
Clinical presentation
Unlike with testicular torsion, the pain is typically more gradual in nature, although you must still thoroughly exclude testicular torsion from your differential. If there is an overlying UTI you may also expect UTI symptoms (FUND – frequency, urgency, nocturia, dysuria). Screen for risky sexual behavior and new partners as well.
Similar to torsion however, there may also be unilateral scrotal pain and swelling. Due to its infectious etiology the patient may also present with a fever, although this is not necessary. On exam you may notice a positive Prehn sign which may help distinguish it from torsion.
Diagnosis
Epididymitis is a clinical diagnosis, but can be supported with lab work. Consider ordering:
- CBC to look for elevated WBC
- Urinalysis to look for nitrites and leukocyte esterase
- STI testing
- U/S if an abscess is suspected (patient looks really sick) or if you cannot confidently rule out torsion. Doppler U/S would show increased blood flow (instead of decreased in torsion) to the affected testis
Management
Provide antibiotics based on the underlying cause (UTI, chlamydia, gonorrhea). Abscess drainage if necessary. May evolve into sepsis if not treated.
Hydrocele
To understand hydrocele we have to understand a very tiny amount of embryology regarding the descent of the testes. This occurs in stages starting from the second month of pregnancy all the way till birth.
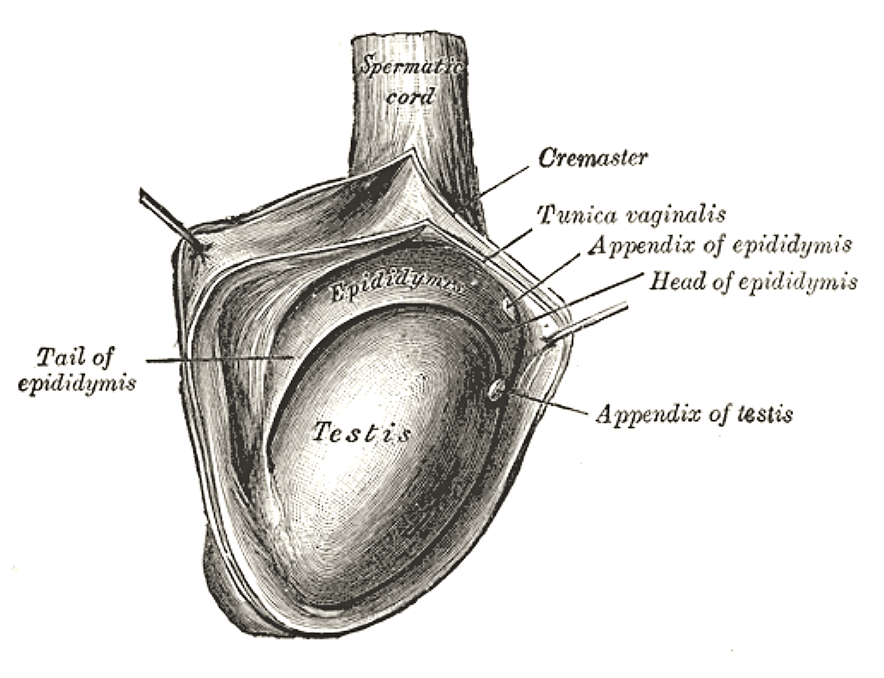
Initially the testes are connected by 2 ligaments: cranially by the cranial suspensory ligament and caudally by the gubernaculum. Before the testes can descend into the scrotum, the peritoneum invaginates caudally towards the gubernaculum forming the processus vaginalis. Under the influence of androgens, the cranial suspensory ligament regresses allowing the gubernaculum and gravity to pull the testes down into the scrotum. As the testes drops into the scrotum it passes behind the processus vaginalis. After the testes have dropped, the processus vaginalis becomes obliterated proximally but a remnant of it remains surrounding the testis, this remannt is called the tunica vaginalis. The tunica vaginalis now serves as a pouch that covers the testes. The obliterated processus vaginalis will remain a weak spot for intestines to herniate into causing inguinal hernias.

https://www.youtube.com/watch?v=6PcerMP9bFM
In hydrocele, there is the accumulation of fluid in the tunica vaginalis, which essentially means in hydrocele that is fluid surrounding the testes testis and compressing it. It is most commonly due to an unknown cause however it can also be related to trauma, iatrogenic injury, tumor or torsion. If it occurs in neonates or infants, it may also be due to the congenital failed obliteration of the processus vaginalis that occurs prior to birth (this would be considered a communicating hydrocele, since the passageway between the peritoneal cavity and scrotum is still open).
Clinical presentation
Often asymptomatic, painless swelling of the testes. Palpation would reveal fluctuant swelling and no pain.
Diagnosis
Clinical diagnosis that can be confirmed with U/S.
Management
In infants it will spontaneously resolve by 6 months after birth. In adults, if there is no pain no surgery is needed. If swelling is becoming a source of discomfort or may be affecting fertility surgical excision of the sac or aspiration of the fluid within the sac may be warranted.
Varicocele
To understand varicocele we have to understand a very tiny amount of testicular anatomy. The spermatic cord connects each testis to the rest of the body. Major vascular components of the spermatic cord include the testicular artery, the vas deferens veins and the pampiniform plexus.
There are 2 main causes of varicocele:
- The blood from the pampiniform plexus drain into the testicular veins which contain one-way valves which support the flow of the venous blood back to the heart. If these valves are damaged it can result in a varicocele as blood flows backwards back into the testicle. The left testicular vein is longer than the right one, which leads to greater intravascular pressures on the left side than the right.
- The left testicular vein drains into the left renal vein at a 90 degree angle. Unfortunately, the superior mesenteric artery passes on top of the left renal vein and in some patients can compress the left renal vein. This compression not only causes blood to pool back in the kidney causing renal hypertension, but it also causes inadequate drainage of blood from the left testicular vein into the left renal vein. This phenomenontermed “nutcracker syndrome” can result in left varicocele.

https://www.youtube.com/watch?v=d4_LnU43yzU
Because of the nutcracker syndrome and the fact that the left testicular vein is longer, varicocele more commonly occurs in the left testicle than the right!
As a result of the backflow of blood into the pampiniform plexus, this causes the plexus to become swollen and varicose veins to form in this plexus.
Clinical features
Patients may complain of a painless enlargement similar to a hydrocele, or they may also complain of an aching pain. Patients may also have a history of infertility as the increased swelling and blood pooling around the testicles provides a higher than normal temperature required for the development of sperm.
On exam, the classic feature of the affected testis when palpated is a bag of worms feel. The swelling and pain may get worse when standing or bearing down, and better when supine.
Diagnosis
Ultrasound can identify varicose plexus.
Management
If there are no symptoms or minimal symptoms then no surgery is required. However, if there is pain of it is affecting fertility, surgery can be performed to embolize or ligate the varicose veins.
Appendix testis torsion
Unlike testicular torsion appendix testis torsion is not a surgical emergency. It results when the hydatid of Morgagni which is an embryological remnant found on the anterioposterior surface of the testis rotates on itself causing ischemia, tenderness and symptoms resembling a testicular torsion.
Clinical features
Appendix testis torsion more commonly affects younger boys between 3 – 7 years old.
If you on exam you observe the blue dot sign then this is pathognomonic for appendix testis torsion as the blue represents the infarcted appendix.
Diagnosis
Clinical diagnosis which can be supported with an ultrasound.
Management
Surgical intervention is typically not necessary, and NSAIDs, ice and rest can be used to manage the pain and swelling.
Testicular cancer should always be on your mind for a patient with a painless firm or hard mass!