The list of diseases and conditions that causes vomiting and diarrhea in the pediatric population is diverse. There are diseases that range from exclusively affecting newborns to those that manifest later in life, and diseases that require urgent surgical intervention to conditions that require simply changing the infant’s nutritional intake.
Milk protein-induced enterocolitis (MPIE)
Milk protein-induced enterocolitis occurs in infants who consume formula who are allergic to milk protein.
Age: commonly age when formula is introduced
Clinical presentation of infants with MPIE is vomiting and diarrhea that usually follows the introduction of formula into the diet. However, it may also occur in infants who are breastfed by a mother who is consuming milk products, and the milk proteins can pass into the breast milk. Infants with MPIE may also present with failure to thrive (weight loss) and dehydration. Stool will be occult blood positive and may also have gross blood.
Management is simple with avoidance of products containing milk protein. Mothers breastfeeding most also avoid milk protein products.
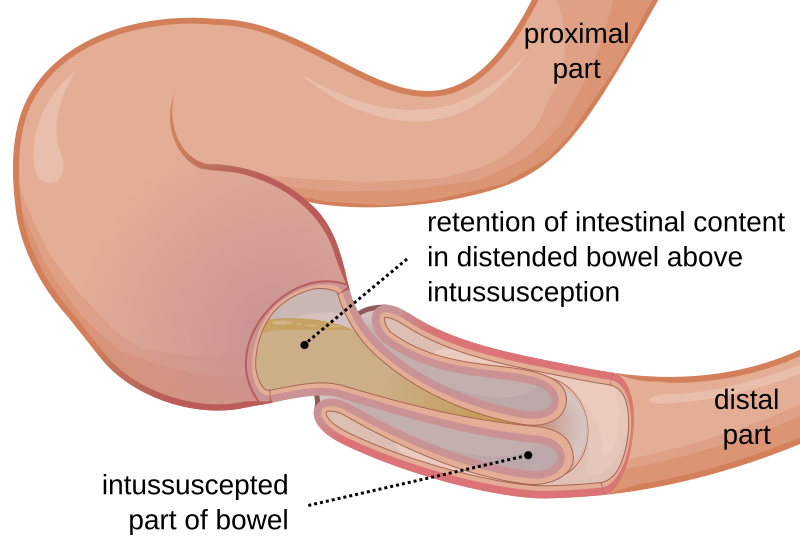
Intussusception
Intussusception is when the proximal part of the small intestine protrudes into a more distal part of the small intestine causing a retention of the intestinal content in the proximal intussucepted part of the bowel.
Age: 3 months to 3 years (rare in neonates)
Clinical presentation of infants is a triad of vomiting, abdominal pain and bloody stool. The bloody stool is classically referred to as currant jelly stool which means it looks like stool mixed with blood and mucus. Abdominal pain is described as acute, severe and colicky with the infant often drawing their knees to the chest. The vomitus is usually initially non-bilious. Another classic sign of intussusception is a palpable RUQ mass on abdominal examination.
Triad of intussusception is vomiting, abdominal pain, and currant jelly stools!
Diagnosis is with a x-ray or ultrasound, with a CBC and electrolytes to look for signs of dehydration or blood loss.
Management is first directed at replenishing the fluid loss with fluid resuscitation and possibly nasogastric decompression of stomach contents. Next step would be an air enema to resolve the intussusception, although this should be avoided in patients with peritonitis. Open or laparoscopic surgical management may be needed since intussusception is a surgical emergency, with complications of bowel necrosis and perforation if untreated.
Midgut volvulus
Midgut volvulus is a disease that is a consequence of intestinal malrotation during fetal development. The malrotated midgut is predisposed to torsion (twisting of a loop of bowel on its mesentery) which is a surgical emergency. Common cause of intestinal obstruction in this age group.
Age: neonates – first few months after birth
Clinical presentation involves bilious emesis, colicky abdominal pain and abdominal distention.
Diagnosis should include a CBC, lactate and electrolytes to assess for blood loss, electrolyte imbalance from emesis, and volume depletion. An upper GI series with oral contrast is the standard for any infant with new onset acute bilious emesis.
Management involves fluid resuscitation and definitive treatment is via emergent surgery (Ladd procedure).
Triad for midgut volvulus is abdominal distention, abdominal pain and bilious emesis!
Necrotizing enterocolitis (NEC)
Necrotizing enterocolitis is a disease involving the hemorrhagic inflammation of the colon in low birth weight or premature infants. Its cause is not entirely known. It is a common cause of acute abdomen in premature infants.
Age: premature infants during the 2nd – 4th week
Clinical presentation typically involves an infant with a distended abdomen who appears very sick, and has signs of shock, fever and hypothermia. These children look very sick! They may also have bloody stools and be difficult to feed. Signs of peritonitis and shock will be seen if it progresses to intestinal perforation.
Diagnosis should start with a CBC to look for inflammation/infection, INR/aPTT to look for DIC and an ABG to look for metabolic acidosis associated with the necrotic bowel. Imaging should include abdominal x-ray and if necessary ultrasound.
Management should start with stopping enteral feeding (with TPN to substitute) and nasogastric decompression. IV broad spectrum antibiotics should also be initiated. Pediatric surgery should be consulted to assess for bowel excision.
Duodenal atresia
Duodenal atresia is when there is a complete occlusion of the duodenum resulting in the duodenal obstruction. It is a congenital anomaly.
- Atresia: complete occlusion
- Stenosis: narrowing but not complete occlusion
Age: first or second day after birth
Clinical presentation is marked by bilious vomit on the first or second day after birth if occlusion is complete (atresia), and within the first week if the occlusion is incomplete (stenosis). There may also be a delay in the passage of the meconium, the first stool that the infant produces. It is commonly associated with Trisomy 21 (Down syndrome).
Diagnosis is with an abdominal x-ray which will show the classic double bubble sign as air and fluid builds up proximal to the duodenal obstruction, resulting in 2 bubbles on x-ray. One bubble in the stomach (which is normal) and one bubble in the duodenum (which is abnormal). The two bubbles are separated by the pyloric sphincter.
During the intrauterine phase polyhydramnios (excess of amniotic fluid due to increased production or decreased resorption) will also be present as the infant is unable to swallow the amniotic fluid.
Management should first involve fluid resuscitation, TPN, and nasogastric decompression with surgery for definitive treatment.
Hirschsprung disease (congenital aganglionic megacolon)
Hirschsprung disease is a congenital, inherited disease that is characterized by aganglionic colon segment (rectosigmoid region). This segment is unable to relax which leads to a functional (but not structural) intestinal obstruction.
Age: neonates
Clinical presentation is marked by the delay passage of the meconium which should pass within 48 hours after birth as well as abdominal distention and bilious vomiting.
Diagnosis is using imaging such as abdominal x-rays and barium enema. Confirmation with rectal biopsy.
Management involves definitive treatment by surgical resection of the aganglionic segment. If Hirschsprung disease is left untreated it can progress to Hirschsprung enterocolitis where the infant develops pain, fever and foul and bloody smelling diarrhea which can progress into toxic megacolon and sepsis.
Clinical presentation: delayed passage of meconium, abdominal distention and bilious vomiting!
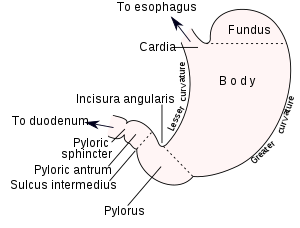
Pyloric stenosis
Pyloric stenosis involves the rapid hypertrophy and hyperplasia of the pyloric sphincter after birth.
Age: 2nd to 7th week after birth
Clinical presentation is marked by the production of nonbilious emesis projectile vomiting. Presents with failure to thrive.
Diagnosis should start with a CBC and electrolytes to look for electrolyte imbalance and dehydration. Due to constant vomiting these patients may have hypokalemic and hypochloremic metabolic alkalosis. Next palpation and US should be performed to look for an olive shaped structure in the epigastrium which represents the hypertrophy of the pylorus. Barium swallow studies are NOT required.
Management involves fluid and electrolyte replacement, frequent and small meals and definitive surgery with Ramstedt pyloromyotomy.
BILIOUS VOMITING is seen in midgut volvulus, duodenal atresia and Hirschsprung disease!